Bronchial Washings Cytology: Diagnostic Use in Lung Infections and Tumors
What is Bronchial Washings Cytology?
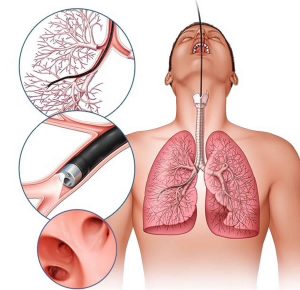
Bronchial Washings Cytology, also known as Bronchial Aspirate Cytology, is a diagnostic cytological evaluation of cells obtained from the bronchial tree during bronchoscopy. It helps detect infectious agents, tumors, and inflammatory processes.
Synonyms
- Bronchial Aspirate Cytology
- Bronchial Wash Cytology
- Tracheal Aspiration Cytology
Specimen & Collection
- Specimen: Bronchial washings or tracheal aspirates
- Container: 50 mL disposable centrifuge tube
- Collection Method: Inject 3–5 mL of physiologic saline through a bronchoscope and aspirate the fluid during bronchoscopy.
- Post-Care: Collect sputum post-procedure for better cytologic yield.
Patient Preparation
Ensure informed consent is obtained for bronchoscopy. Consider patient immunocompromised status and inform the lab accordingly.
Sample Handling Instructions
- Labeling: Accurate labeling is critical.
- Transport: Send immediately to the lab; refrigerate if delay is expected (after working hours).
- Rejection Criteria: Incorrect labeling or room temperature storage for over 6 hours.
Special Instructions
Include clinical history, suspected infections, immune status, imaging results, history of chemo/radiation, and required stains. All specimens are handled under universal precautions.
Test Procedure
After centrifugation, cytospin and membrane filtration techniques are used to prepare:
- Direct smears
- Cell blocks
- Cytocentrifuge (cytospin) slides
Both membrane filtration and cytocentrifugation may be used to optimize diagnostic yield.
Uses
This test is used to detect:
- Primary or metastatic lung tumors
- Infectious agents: Herpesvirus, CMV, measles, fungal infections, Pneumocystis jirovecii (carinii), Strongyloides, Paragonimus
- Opportunistic infections: Especially in AIDS or transplant patients
- Other conditions: Lipoid pneumonia, hemosiderosis (Goodpasture’s syndrome), allergic lung disease, and asbestos exposure
Limitations
Specimens without respiratory epithelial cells are considered unsatisfactory for cytologic interpretation.
Stains and Techniques
Special stains may be needed for better organism identification:
- Ziehl-Neelsen: Acid-fast bacilli (e.g., TB)
- Grocott’s methenamine silver: Fungi (e.g., Pneumocystis)
- Diff-Quik or Giemsa: General morphology and fungi
- Immunoperoxidase & Immunofluorescence: For specific markers and infections
Turnaround Time
Usually within 1–2 days depending on required stains and complexity.
References
- Broaddus C, et al. Ann Intern Med. 1995; 102:747-52.
- Chandler FW, Watts JC. Pulmonary Pathology. Springer-Verlag, 1988.
- Chandra P, et al. Acta Cytol, 1988; 32:105-8.
- Wheeler TM, et al. Acta Cytol, 1988; 32:647-50.
- Jacobs, Demott, Finley, et al. Laboratory Test Handbook, Lexi-Comp Inc, 1994.